
前回のお話はどうだったかな?あの子はODらしくないよね。診断は?という話になるとちょっと説明が必要になる。なぜって、今僕がやろうとしていることは、診断名を当てはめることではなくて、状態を動的なものとして理解し表現することだから。ああ、君のあっけに取られた顔が目に浮かぶ。まだ、閉じないで!ここからが良いところ。
前回、Salience(サリエンス)という言葉をいきなり使いました。そう、身体感覚や出来事に対する重要度を調整する脳のネットワーク機能のこと。これは神経生理学や心理学でよく使われている概念らしいのだけれど、あまり聞いたことはないよね。以下が概要(M作図)。
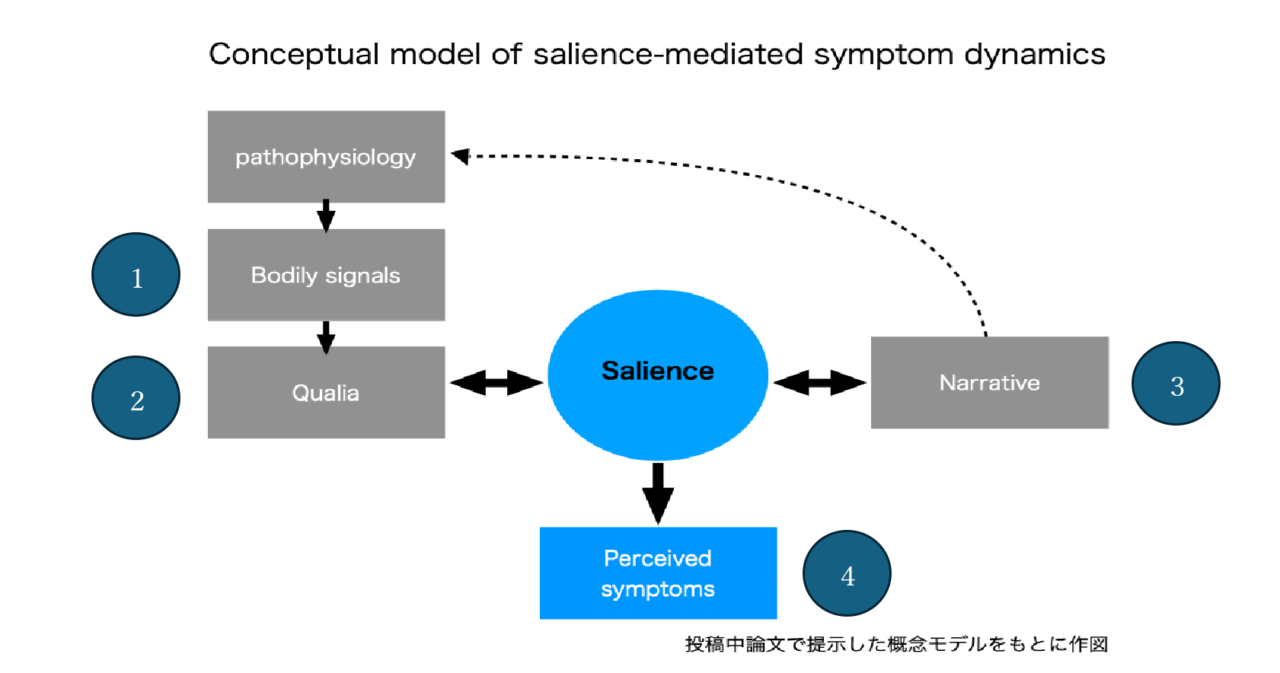
要すれば、①身体(Pathophysiology)から発したシグナルが(Body signals)が、②感覚として感知される(Quolia)が、これは直接症状として現れるのではなくて、Salienceという調整機能で③その人の物語(Narrative)にある価値や感情との間で、④重みづけがなされ症状として現れる(Perceived symptoms)というわけ。しかも身体的なシグナルやnarrativeの変化で動的に調整され、症状が変動するということ。症状に対する重みづけ、意識が変わる。
この子の場合、①就寝時の姿勢による筋刺激 ②後頭部の筋痛 ③妹と母と私/ ダンス ④鈍い頭痛、という状態として理解できるのだ。彼女の物語性に影響を受けた後頭部痛に対する重みづけが大きくなった頭痛。ある物語“母と共にダンス教室へ行く”は症状への注意を減らす。このようにSalienceの動的なシステムから考えると、① 寝る体勢を変える②カロナール処方③ダンスの物語の日常化が現実の介入として考えられる訳だ。また、この症状は病気ではなくて筋肉痛に敏感なだけだ、と説明することで、なんとnarrativeはさらに変容し、注意が小さくなる。家族会議より、心理学的なアプローチより良いでしょ? PCCM的には病いの回復だね。
CMS位置:理解/身体×物語×時間/Salience
How was the previous story? She didn’t quite look like a typical case of orthostatic dysregulation, did she? Once we begin to ask about diagnosis, a certain explanation becomes necessary. That is because what I am attempting here is not to fit a diagnostic label, but to understand and express a state as something dynamic. I can almost see your surprised face. Don’t close this yet—this is where it becomes interesting.
Last time, I suddenly introduced the word salience. It refers to a brain network function that regulates the importance assigned to bodily sensations and events. The concept is widely used in neuroscience and psychology, though perhaps unfamiliar in everyday clinical conversation.
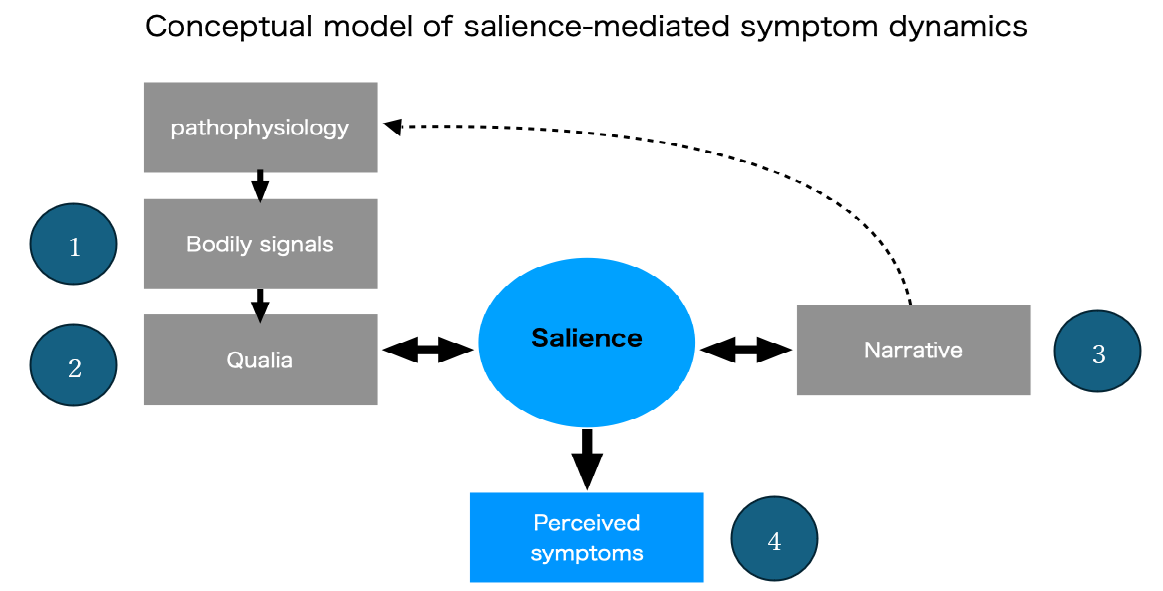
(figure: Salience-mediated Symptom Dynamics)
In essence: (1) signals arising from the body (pathophysiology) are sensed as (2) qualia; yet these do not appear directly as symptoms. Instead, through the regulatory function of (3) salience, they are weighted in relation to the person’s narrative—its values and emotions—and thus (4) emerge as perceived symptoms. Moreover, as bodily signals and narrative context change, this weighting is dynamically recalibrated, and symptoms fluctuate. The very attention given to symptoms shifts.
In this girl’s case, the state may be understood as: (1) muscular stimulation from sleep posture; (2) occipital muscle pain; (3) narrative involving sister, mother, physician, and dance; (4) dull headache. Her headache reflects increased weighting of occipital pain shaped by her narrative context. A different narrative—going with her mother to dance class—reduces attention to the symptom. Seen from this dynamic salience system, practical interventions naturally follow: (1) adjust sleep posture; (2) prescribe acetaminophen; (3) allow the dance narrative to become part of everyday life. Furthermore, simply explaining that this is not an illness but a sensitivity to muscle soreness transforms the narrative itself, and attention diminishes even more. Better than a family conference or purely psychological approach, isn’t it? In PCCM terms, this is recovery of illness.
CMS Position: Understanding / Body × Narrative × Time /Salience
コメント